Last updated on April 24th, 2026 at 09:13 am
Medically responsible content note:
This article is for education only and does not diagnose or treat medical, dental, or sleep conditions. Bruxism, jaw pain, headaches, snoring, breathing pauses, and respiratory symptoms can have multiple causes. Seek care from a qualified medical, dental, sleep, or orofacial pain professional when symptoms are persistent, worsening, severe, or disruptive.
If your oxygen level drops overnight on a pulse oximeter, it is easy to assume you have sleep apnea.
That reaction is understandable. Low oxygen during sleep can be serious. But an SpO2 reading by itself does not tell you what caused the drop, how often breathing events happened, or whether the problem was actually sleep apnea.
That is the key point:
SpO2 is not diagnostic for sleep apnea without other sleep parameters.
A pulse oximeter can still be useful. It may raise suspicion, support follow-up, and help show trends over time. But by itself, it does not provide enough information to diagnose sleep apnea or define treatment success.
If you want the foundation first, start with what obstructive sleep apnea is.
Why this question matters
Sleep apnea, snoring, and other forms of sleep-disordered breathing can affect much more than your nights. They may contribute to daytime sleepiness, poor concentration, morning headaches, low energy, and reduced work performance. Over time, untreated sleep-disordered breathing may also overlap with broader health concerns.
That is why the testing pathway matters. Before treatment such as CPAP or oral appliance therapy begins, the diagnosis should be based on the right kind of sleep data.
If you are unsure whether testing is warranted, review the signs you may need a sleep study.
Screening tools and diagnostic tests are not the same
This topic causes confusion because people often treat screening tools and diagnostic tests as if they do the same job.
They do not.
A screening tool may suggest that a problem is present. A diagnostic test provides enough information to identify the problem with greater confidence and guide treatment decisions.
Pulse oximetry is best understood as a limited physiologic measurement. It can show overnight oxygen and pulse trends, but it does not collect the full range of breathing and sleep data needed to diagnose sleep apnea on its own.
That is why pulse oximetry may be helpful in screening, but it should not be mistaken for a complete sleep apnea test.
For the bigger picture, see how sleep apnea is diagnosed.
What pulse oximetry actually measures
Pulse oximetry estimates peripheral capillary oxygen saturation, or SpO2. In simple terms, it estimates how much oxygen is attached to hemoglobin in the blood.
This can be useful because oxygen desaturation often shows up during sleep-disordered breathing events. A clinician may review those patterns to decide whether additional testing is needed.
But oxygen saturation is only one part of the picture.
A pulse oximeter does not directly measure:
- airflow
- respiratory effort
- sleep stages
- arousals
- actual sleep time
Without those measurements, an SpO2 reading cannot tell the whole story.
For a related topic, see shallow breathing during sleep.
Why SpO2 alone is not enough
This is the central message of the article:
SpO2 is not diagnostic for sleep apnea without other sleep parameters.
A person may desaturate during sleep for several reasons. Obstructive sleep apnea is one possibility, but it is not the only one. Low oxygen during sleep may also be influenced by chronic lung disease, asthma, COPD, cardiovascular issues, body position, motion artifact, low baseline oxygen saturation, or poor signal quality.
Even when the drop is real, oxygen data alone cannot tell you whether the problem was obstructed airflow, reduced airflow, another respiratory issue, or a technical limitation in the recording.
That is why SpO2 can be useful without being diagnostic on its own.
To widen the discussion, explore how respiratory health affects sleep quality.
What a pulse oximeter can and cannot tell you
A simple comparison helps clarify its role.
A pulse oximeter can show:
- oxygen saturation trends
- pulse rate trends
- possible overnight desaturation patterns
- change over time from one night to another
A pulse oximeter cannot show:
- airflow
- respiratory effort
- sleep stage
- true apnea-hypopnea index
- why oxygen dropped
- whether the patient was asleep during each event
That gap is exactly why a pulse oximeter cannot diagnose sleep apnea by itself.
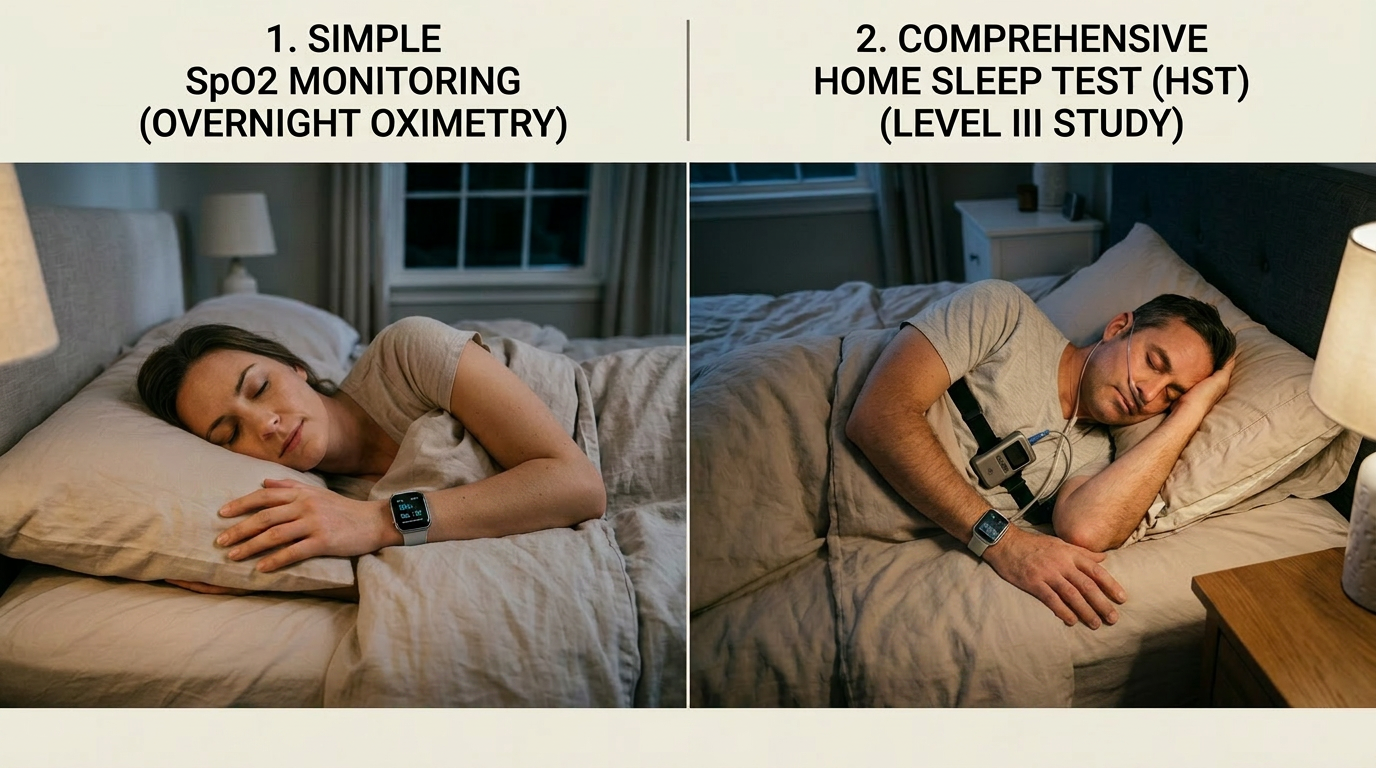
Why a home sleep test gives a clearer answer
A home sleep test provides more clinical value because it measures more than oxygen saturation alone.
For example, a device such as the Nox T3 can collect multiple respiratory signals that help a clinician assess the pattern and severity of sleep-disordered breathing. Depending on the setup, a home sleep test may record:
- airflow
- respiratory effort
- oxygen saturation
- pulse rate
- snoring
- body position
That added context matters. A clinician does not just need to know that oxygen dropped. The clinician needs to know what was happening with breathing at the same time.
That is why a home sleep test offers a much stronger diagnostic pathway than standalone overnight oximetry.
If you are comparing options, read home sleep test vs lab sleep study.
Why PSG still matters
In-lab polysomnography, or PSG, remains the gold standard for sleep diagnostics because it captures the broadest range of sleep-related signals. Depending on the study, PSG can include brain wave activity, eye movement, muscle activity, heart rhythm, oxygen saturation, airflow, and breathing effort.
This wider data set allows clinicians to evaluate much more than oxygen levels and diagnose a broader range of sleep disorders.
For some patients, especially those with more complex symptoms, PSG is the better test.
Where WristOX2 fits
The WristOx2 is a good example of a pulse oximetry device that can still be useful in the right setting. It can collect overnight oxygen saturation and pulse trends in a convenient home environment.
That may help with:
- physiologic trend review
- screening suspicion in some workflows
- follow-up support
- adding context to a broader sleep evaluation
But the limitation remains the same:
WristOx2 data alone does not diagnose sleep apnea.
Without airflow, breathing effort, and other sleep parameters, the device cannot define the nature of respiratory events or confirm severity the way a true sleep test can.
How SpO2 can help during oral appliance titration
Although SpO2 is not diagnostic by itself, that does not mean it has no treatment value.
In dental sleep medicine, overnight oximetry can serve as a non-diagnostic outcome metric during the titration phase of oral appliance therapy. In practical terms, a dentist may compare oxygen trends and desaturation patterns before and during mandibular advancement to see whether the appliance appears to be moving in the right direction.
That does not replace a follow-up HST or PSG, and it does not prove treatment success on its own. Proper medical follow-up testing is still needed to confirm efficacy.
What overnight SpO2 can do is provide an early signal that things may be improving. If oxygen trends look better, desaturations appear less severe, or the overnight pattern looks more stable, that information may help support titration decisions before the patient returns for formal follow-up testing.
Used this way, pulse oximetry functions as a practical, lower-cost checkpoint rather than a diagnostic endpoint.
Why that can matter financially
Titration takes time. Advancing an oral appliance too little may leave symptoms unresolved. Advancing it too far may increase side effects, discomfort, or bite changes.
Because of that, dentists often need some way to judge whether treatment appears to be moving toward a better physiologic result before ordering a follow-up home sleep test or lab study.
This is where SpO2 can be useful. As a non-diagnostic metric, it may help identify whether the patient seems to be trending toward improvement. That can support more informed titration adjustments and may reduce the need to repeat formal testing too early in the process.
In some cases, that can save a tremendous amount of cost by helping the team avoid unnecessary repeat diagnostic-grade studies before the appliance is close to an effective position.
The distinction still matters:SpO2 may suggest improvement, but it does not confirm treatment efficacy.Confirmation still requires appropriate follow-up testing.
Why Nox T3 is a better example of a sleep apnea test
If the question is whether someone has sleep apnea, the Nox T3 is a much better example of a proper home testing pathway.
That is because it is designed to gather multiple respiratory signals, not just oxygen saturation. It provides a more complete picture of what happens during sleep and gives clinicians a better basis for interpretation.
This is the difference between asking, Did oxygen drop? and asking, What happened to breathing during sleep?
Those are not the same question.
Why you cannot calculate AHI from SpO2 alone
The diagnosis and classification of sleep apnea often rely on the apnea-hypopnea index, or AHI. That number depends on identifying breathing events over time.
A standalone pulse oximeter cannot do that reliably because it does not directly measure airflow reduction, breathing effort changes, or actual sleep time.
A suspicious desaturation pattern may point toward a problem. But suspicion is not the same as diagnosis.
The same logic applies during treatment. Better overnight SpO2 trends may suggest progress, but they are not the same as a documented post-treatment AHI or other formal outcome measure derived from proper sleep testing.
To connect this back to the condition itself, see what obstructive sleep apnea is and how it is diagnosed.
Why overnight oxygen readings can mislead you
Pulse oximetry is widely used, but like any tool, it has limitations. Overnight SpO2 readings can be affected by:
- poor perfusion
- movement during sleep
- nail polish or acrylic nails
- signal dropout
- ambient light interference
- improper sensor placement
This matters even more in unattended home use, where no technician is present to correct problems in real time.
A low reading should not be ignored. But it also should not be treated like a complete diagnosis. The same caution applies in reverse: a better-looking SpO2.night does not automatically mean the sleep apnea is fully treated.
When pulse oximetry still has real value
None of this means pulse oximetry is useless. It is not. It can still be a helpful part of the process when used for the right purpose.
Pulse oximetry may help with:
- identifying suspicious desaturation patterns
- adding physiologic context
- supporting follow-up
- monitoring trends over time
- helping determine whether more complete testing is needed
- providing a non-diagnostic titration checkpoint during oral appliance therapy
It is a useful piece of the puzzle. It is just not the whole puzzle.
A better pathway for patients with symptoms
If a person snores, wakes unrefreshed, feels very tired during the day, develops morning headaches, or has witnessed pauses in breathing, the next step should usually be more than overnight SpO2 alone.
A stronger pathway is to:
- review symptoms and risk factors
- use screening tools such as STOP-Bang or the Epworth Sleepiness Scale
- move to home sleep testing, such as a Nox T3, or to in-lab PSG when appropriate
- begin treatment when indicated
- use careful titration and symptom review
- confirm the treatment result with proper follow-up testing
That approach is more efficient and more clinically sound than assuming oxygen data alone gives the full answer.
If headaches are part of the picture, see why sleep apnea can cause morning headaches.
Bottom line
Pulse oximetry is useful, convenient, and easy to use. Devices such as the WristOx2 can provide meaningful overnight oxygen data.
But the main point should stay clear:
SpO2 is not diagnostic for sleep apnea without other sleep parameters.
A pulse oximeter does not measure airflow, respiratory effort, sleep stages, or enough information to define the nature and severity of breathing events on its own.
At the same time, overnight SpO2 can still be useful in dental sleep medicine as a non-diagnostic metric during oral appliance titration. It may help show that a patient is moving toward a better physiologic outcome before follow-up HST or PSG testing is performed.
Used appropriately, that kind of interim feedback may help guide titration more efficiently and, in some cases, reduce unnecessary cost. It should never be confused with formal confirmation of treatment success.
If the goal is to diagnose sleep apnea or document treatment efficacy, a true sleep test such as a home sleep test with a device like the Nox T3 or an in-lab polysomnogram remains the better option.
Take a low overnight oxygen reading seriously. Just do not mistake one signal for a complete diagnosis.
FAQ
Can a pulse oximeter diagnose sleep apnea?
No. A pulse oximeter can show overnight oxygen patterns, but SpO2 alone is not diagnostic for sleep apnea without other sleep parameters.
Can dentists use SpO2 during oral appliance titration?
Yes, but only as a non-diagnostic metric. Overnight SpO2 may help dentists look for improvement trends during titration, but it does not replace follow-up HST or PSG testing.
Can improved overnight SpO2 prove that oral appliance therapy is working?
No. Better oxygen trends may suggest improvement, but they do not confirm treatment efficacy on their own.
Why might dentists use overnight oximetry before follow-up HST or PSG?
It may help guide titration decisions, show whether the patient appears to be trending in the right direction, and reduce the need for repeat formal testing too early in the process.
Is WristOx2 a sleep apnea test?
WristOx2 is a pulse oximetry device that can provide overnight oxygen data, but it does not diagnose sleep apnea on its own.
Is Nox T3 a home sleep test device?
Yes. Nox T3 is a home sleep testing device that can record multiple respiratory parameters and provide more useful clinical information than SpO2 alone.
What is the difference between pulse oximetry and a home sleep test?
Pulse oximetry measures oxygen saturation. A home sleep test measures oxygen saturation plus other parameters such as airflow, respiratory effort, and body position.
What is the gold standard test for sleep apnea?
Polysomnography, or PSG, is the gold standard because it records the broadest range of sleep-related parameters.
Author Disclaimer from Randy Clare: I mention the Nox T3 and WristOx2 in this article because they are devices I came to know well earlier in my career, and they serve as useful examples for explaining the differences between overnight oximetry and sleep testing. I do not receive compensation from the companies behind these products, and neither does The Sleep and Respiratory Scholar. I am using them strictly as familiar reference points to help make the topic clearer for readers.

Randy Clare is a writer, educator, and health communicator focused on making complex clinical topics easier to understand. Through The Sleep and Respiratory Scholar, he creates clear, practical content on bruxism, headache, sleep, airway health, and respiratory symptoms. He is the author of The Brux Method, President of ClenchAlert.com and host of The Clenching Chronicle Podcast, where he explores jaw tension, clenching, headaches, and behavior-based approaches to relief. His work helps readers better understand symptoms, recognize patterns, and take more informed next steps.